Many women face a choice between career advancement or motherhood. But emerging fertility technologies could allow women to have it all.
The gender pay gap has barely changed since the early 2000s. In the US women who work full time earn 84 percent of what men earn. Twenty years ago they earned 80 percent. One of the main reasons for this is that women spend a lot of time bearing and caring for children, especially during their early years. This work provides significant public benefit, but it comes at a private cost: women’s wages drop after giving birth and never fully recover.

Women know this gap exists and plan accordingly: in countries where the motherhood penalty is keenest, the birth rate is lower.
Subscribe for $100 to receive six beautiful issues per year.
Governments have worked to address gender pay gaps by introducing maternity and paternity leave, creating preschool programs, providing tax benefits to parents, and more. These policies have helped, but they are limited in what they can achieve so long as women continue to have children during the years most critical to their careers.
Taking time out of the workforce to bear and raise children while in their twenties and thirties means women have less time to accumulate the network, skills, and experience necessary to rise to the top of their fields. The later women wait to have their first child, the more they earn.

But unfortunately, women’s fertility falls with age. If women wait until they are 40 to have children, they can probably achieve the career they want, but they are unlikely to have as many children as they would like – and they may not be able to have children at all. How to manage this tradeoff is a pressing question for any woman in the modern world. But emerging technology may solve this problem.
In fact, this may be a unique few decades of history where women have the option to choose professional accomplishment but risk (unwanted) childlessness as a price. New technology may soon allow women to maintain their fertility into their forties and fifties, giving them the same options that men have.
The motherhood pay gap and greedy careers
People choose their careers for more than just money. They also want to gain respect, do interesting work, and have a positive impact. However, the top of many careers is where the most rewarding and influential work is done, and women face not just a pay gap but an overall career gap. They make up under a third of the American C-suite, just over a third of principal investigators leading academic science projects, and only 26 (out of 100) US Senators.
We have come a long way from the explicit sex discrimination of the past. Today, the gap is primarily driven by the career toll exacted by motherhood.
Mothers around the world continue to invest more time in childcare than fathers do. In the US, for example, women with children under six spend 36 hours on average in domestic activities, compared to 18 hours for men. This pattern holds true even when both parents are working full time.
This time investment does not hurt women in fields with constant returns to hours – where each hour worked is about as productive on average as the last hour worked, like fast food workers or pharmacists.
But the gap does hurt women in ‘greedy careers’ – careers that are greedy for the employee’s time and pay more per hour to the people who work the most. Consider a corporate lawyer working on a deal. The initial hours are spent getting familiar with the material and the people involved. Later hours – once the lawyer understands the case – are much more productive than those at the start. A person working a 40-hour week in this scenario does more than twice as much work as a person working a 20-hour week. Lots of careers are like this.
Executives and managers have particularly greedy jobs, and as such, the motherhood career gap is especially pronounced in these roles. One study found that, for their first few years, graduates from the University of Chicago’s Booth School of Business (between 1990 and 2006) worked a similar number of hours – around 60. But by nine years after graduation, an hour’s gap opened up. Women working full time worked an average of 52 hours per week, compared with 58 hours for men. They were much more likely to have taken a break from work (32 percent versus 10), be working part time (15 percent versus 3), or to be not working at all (13 percent versus 1). This was reflected in their earnings, which started slightly lower, grew in step with their male counterparts and then, after eight years, began to plateau and fall.
Academic career paths are another illustration of this ‘leaky pipeline’ problem. Women outnumber men as undergraduates, as master’s degree holders, and increasingly, in PhDs, but they are outnumbered by men in postdoctoral positions. The gap widens in faculty roles, and especially in senior leadership – positions that women usually apply for after becoming mothers.
A race against time
Many women, especially highly educated women, see this tradeoff and decide either never to have children or to have fewer than they would ideally want. This is a high price to pay. Society as a whole misses out on both the children that these women would have had and the work that these mothers would have done had they remained in the workforce, a deficit that leads to less innovation and economic growth, higher taxes to support care for the elderly, and lower living standards overall.
Women wishing both to establish their careers and to have children are in a race against time. This is particularly true given that one’s thirties are a particularly defining decade in greedy careers. In law, for example, this is when the highest levels of salary growth take place. Founders who launch unicorns (startups worth more than a billion dollars) have a median age of 34 when they found their companies. In academia, one’s thirties are usually the time when a researcher goes through a string of high-pressure postdoctoral positions in an attempt to secure an independent position.
Aware of this, women often delay pregnancy until they have advanced in their careers as far as possible. This is particularly true for women with PhDs or professional degrees. Women without a bachelor’s degree tend to have 1 to 1.5 children on average by age 28, while those with higher educational attainment have around 0.25 children by the same age. Highly educated women attempt to catch up during their thirties, with their birth rates increasing more rapidly compared to less educated groups. However, this compensatory period is limited, as fertility rates across all education levels tend to plateau around age 39. Thus, the educated group ends up with fewer children despite its members’ attempts to compensate for lost time.
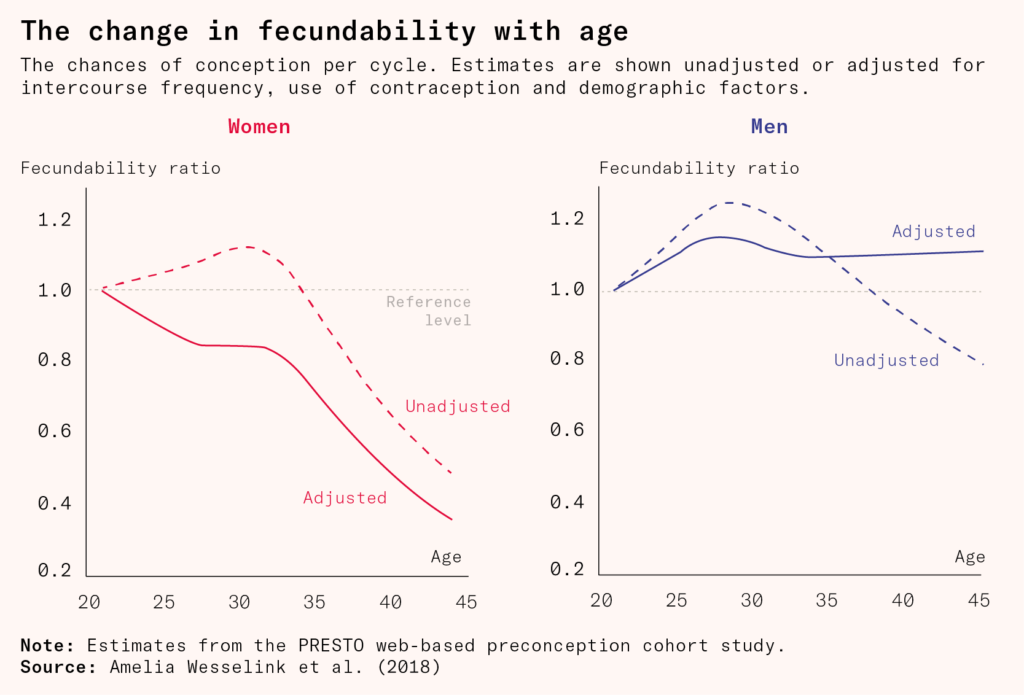
The chance of conceiving a baby naturally with regular sex drops from 25 percent per month in one’s twenties to about five percent per month at 40, while the chance of miscarrying rises from about eight percent for women under 30 to around one in three for 40-year-olds. Around a quarter of women will experience difficulty becoming pregnant in their late thirties, and it’s not yet possible to predict who. And virtually all women become infertile during their forties. This means that women who want biological children often need to plan to have children earlier in life, whether or not it suits their professional desires.
In a survey of 1,056 female doctors in the US, three quarters reported delaying having children despite knowing that fertility declines with age. More than a third of them experienced infertility – defined as failure to achieve a pregnancy after 12 months of regular sexual intercourse – about double the rate for women of all ages trying to conceive, while 19 percent required IVF in order to conceive, at least 1.5 times the population at large. This data mirrors that of other high-stakes careers: women in academia, for example, are less likely than male academics to have children and those who do have fewer children and have them later than women outside academia.
Technology as a solution
People often think that solving problems via biological means is nearly impossible, whereas behavioral and social interventions are merely very difficult. But this isn’t always the case. The social solution to obesity, for example – changing the formula of high-calorie foods, instilling new eating habits in people, and discouraging unhealthy eating – has failed in country after country.
By contrast, semaglutide and other GLP-1 agonist medications have been found to reduce body weight by an average of 20 to 30 percent while reducing the risks of cardiovascular and kidney disease and extending lifespan. After 2020, when they started to be used for weight loss, the adult obesity rate in America began falling for the first time in over forty years.
Preventing the spread of HIV through social interventions was somewhat successful during the 1980s and 1990s, but 450,000 Americans still died of AIDS. And these interventions relied on widespread condom use and HIV testing, both new technologies, not just social change through abstinence. Medical innovations that involve minimal behavioral change, like pre-exposure prophylaxis (aka PrEP), have dramatically reduced the chances of contracting HIV. And while HIV was a death sentence only 40 years ago, advances in antiretroviral therapy mean that people with HIV can now have an expected lifespan that is almost identical to that of the general population if caught early enough.
What if the same were true for the motherhood penalty? Perhaps there are technologies that could extend women’s fertility in the same way that the pill and abortion help them control it.
Expanding the reproductive timeframe for women could also boost birth rates, especially among the most educated who exhibit the largest discrepancy between their intended family size and the actual number of children they have. Consequently, providing these women with an extended window to compensate for their delayed entry into parenthood may lead to an increase in total births.
Freezing eggs
In 2019, Erramatti Mangayamma made headlines when she became the oldest mother on record at 73. The catch: she was not using her own eggs but a younger donor’s. With in vitro fertilization (usually known as IVF), eggs are collected, fertilized in a laboratory, and then implanted in a womb. Women are born with all the eggs they ever get. Reproductive aging in women stems primarily from egg aging, and eventual infertility occurs when they start to run out of eggs. As women age, their chances of conceiving through IVF using their own eggs decreases significantly, but when they use eggs from younger donors, their success rates fall very little. The uterus, it seems, is far less affected by age than the eggs themselves.
For some women, donor eggs are a solution, but many others have a strong preference for raising children who are genetically their own. So far, the only proven way to extend a woman’s fertility window with her own eggs is by freezing those eggs at an earlier age.
The process is straightforward on paper: a young woman’s eggs are collected and stored at minus 196 degrees Celsius to preserve their quality. Then, after years or even decades, the eggs can be thawed and used for conception in a standard IVF process. In essence, egg freezing allows a young woman to become an egg donor for her future, older self. But there is a big difference between theory and implementation.
First, there is the question of whether the process of egg freezing is even efficient. Women have only been freezing eggs in large numbers since 2012, meaning there is much less data on their outcomes than there is for women who use IVF with fresh eggs. The largest study to date is a retrospective 15-year investigation conducted by researchers at NYU Langone Medical Centre, which found that live birth rates using frozen eggs are comparable to live birth rates using fresh eggs of the same age. With the caveat that this is just one study of one fertility clinic, the results are promising: women who froze more than 20 oocytes (immature egg cells) before the age of 38 had a 70 percent chance of having a baby overall. Despite the freezing, storing, and thawing procedures, their frozen eggs seem to act as age-matched, fresh equivalents, which suggests that this process does not massively impair the egg’s ability to lead to a live birth.
However, a number of media reports have been less sanguine about egg freezing. The same NYU Langone study was used as the basis for an article titled ‘The failed promise of egg freezing’, which cites a 39 percent success rate for the procedure. This and other accounts are misleading because they don’t differentiate between women who froze small and large numbers of eggs or between women who froze their eggs at a younger or older age. The result that women can conceive successfully later in life if they freeze enough eggs before they are 38 is important in its own right.
Still, 70 percent is far from a perfect success rate. Many women cannot retrieve 20 eggs or more from just one cycle – the average for women under 34 is around 12 per cycle – and some may fall short of that number even after multiple cycles. So 70 percent is an optimistic figure, and it still leaves almost one in three women involuntarily childless. The egg freezing process is also expensive, costing between $8,000 to $15,000 per cycle. Fortunately, more and more women are being covered by insurance plans that offer free egg freezing. According to a 2021 survey, 20 percent of American companies with over 20,000 employees and 11 percent of smaller companies offer such benefits – an increase from six and five percent respectively in 2015. But most women still have to pay out of pocket.
It’s not just the cost that puts young women off egg freezing. The egg collection process, which involves around two weeks of hormonal stimulation, is often emotionally and physically taxing. About a fifth of women report experiencing severe pain during hormonal stimulation, and virtually all women report some level of pain. And somewhere between 0.1 and three percent of cycles result in severe ovarian hyperstimulation syndrome (OHSS), an overreaction of the ovaries that requires hospitalization and can be fatal if not properly addressed.
Improving egg freezing
Egg freezing would be much better if it were cheaper, less painful, and more efficient.
Egg freezing and IVF rely on highly skilled human technicians to perform delicate cellular manipulations under a microscope. The precise and manual nature of these procedures also introduces the risk of human error and lapses in consistency.
One of the best-funded startups attempting to automate away skilled human labor is Overture Life, which recently published early results from a pilot study using a robot to perform intracytoplasmic sperm injection – injecting a single sperm into an egg – something usually performed manually by highly experienced embryologists.
Overture has also ventured into automating the egg vitrification (flash freezing) and thawing processes with their DaVitri machine. So far, the reported oocyte survival rates look promising but are still lower than those from the manual procedure: 87 percent versus 93 percent.
These early successes are not yet confirmed in larger cohorts or copied across other parts of the egg freezing and fertilization processes, but they show promise for reducing the need for experienced human labor, as does the start-up IVF2.0, one of many companies aiming to use artificial intelligence to select sperm and embryos that are more likely to survive.
The promise of in vitro maturation and in vitro gametogenesis
Most cells in our bodies develop from stem cells and share the same DNA as one another, yet have staggeringly diverse forms and functions. This is possible because, as stem cells mature, they gain epigenetic modifications – modifications on top of or surrounding their DNA – which act as additional instructions on how to interpret their DNA code.
This process is crucial for cells to specialize. It means a liver cell, for example, will ‘read’ its DNA differently from a muscle cell. But once a cell has differentiated into a mature cell, it normally cannot go back to its original stem cell state: except in rare cases, such as during cancer and wound healing, it is locked into its fate.
Cellular reprogramming allows us to modify a cell’s destiny. By adding a cocktail of four proteins to cells in a dish, researchers have been able to reverse a cell’s differentiation and obtain stem cells from mature, specialized cells. These artificially produced stem cells, called induced pluripotent stem cells, can now be differentiated into a whole range of desired cell types, allowing researchers to convert one type of mature cell into another. Since their discovery, pluripotent stem cells have become ubiquitous in medical sciences, facilitating advances that range from gene therapies to better cancer drugs.

Companies such as Gameto and Vitra Labs are working to differentiate pluripotent stem cells into ovarian support cells and recreate an ovary in a lab dish. This would allow doctors to collect immature eggs from a volunteer and then induce them to mature in vitro by placing them in the nourishing environment of the stem cell-derived ‘artificial ovary’. The process is aptly called in vitro maturation (or IVM), as it stands in contrast to the current methodology, wherein eggs mature inside the woman’s body.
The main advantage of IVM is that it allows immature eggs to be collected instead of mature ones, which significantly reduces the burden of hormonal stimulation. Collecting immature eggs can be done with just three days of low-dose follicle-stimulating hormone, often just one jab, compared to 12 days that are required for mature egg collection. This means much less pain, nausea, and constipation. It virtually prevents ovarian hyperstimulation syndrome. What’s more, about 20 to 30 percent of the cost of egg freezing currently comes from fertility drugs, which IVM economizes on dramatically.
The scenario described above involves women opting for minimal ovarian stimulation. But IVM is a versatile technique that could also be used alongside standard IVF to improve its overall efficiency. As it currently stands, around 25 percent of eggs collected during normal IVF rounds are immature and discarded. Being able to use these eggs would offer an important boost to final live birth rates for IVF, primarily helping women who are not able to produce a lot of mature eggs.
In vitro maturation is not a faraway dream. Gameto has started trials to quantify IVM’s ability to rescue those immature eggs that would be discarded in standard IVF. In December, following hormone stimulation requiring only 20 percent of the injections of conventional IVF, the first IVM baby was born.
IVM could be seen as the first step towards achieving something much more ambitious and riskier: the creation of not merely ovarian support cells but actual eggs from stem cells. This approach is called in vitro gametogenesis (IVG), and it would bypass the need for egg freezing entirely. Interest in this technique spiked in 2016 when an academic team in Japan first demonstrated the birth of live mouse pups from eggs produced via IVG. Since then, start-ups like Conception, Vitra Labs, Dioseve, and Ivy Natal have sought to turn IVG into a commercial endeavor for humans.
Translating successes in mice into a reliable method for human oocyte production is not going to be easy. Even in mice, the process has been very inefficient, with only one to three percent of the pluripotent-stem-cell-derived eggs able to produce live pups. And given that oocyte development differs in humans compared to mice in significant ways – including the fact that it takes much longer – translating even this modest level of success between species is not going to be trivial.
But why is this so hard? If we have successfully produced so many types of cells from stem cells, including ovarian support cells, what’s holding us back when it comes to eggs?
Eggs are a very special type of cell. They must contain all of the necessary components to initiate and support the development of an entire new organism, like nutrients, mitochondria, and enzymes, while also providing half of the genetic material for it. They are larger than any other human cell: about 100 microns in diameter, about the same as a strand of hair. They also take much longer to develop. In humans, the process begins before birth and can take decades to complete. Moreover, unlike most cells, which divide by mitosis, egg cells undergo meiosis, a more complex form of cell division that reduces the chromosome number by half. All these factors combined mean that successful differentiation of induced pluripotent stem cells into eggs is a much harder technical problem than obtaining other cell types, including ovarian support cells. However, researchers are taking a shot at it, aiming to use the same proteins (or transcription factors) to guide the development of eggs in culture. In 2024 a team at Harvard announced that it had used this technique to achieve the induction of human meiosis in vitro for the first time.
In-vitro gametogenesis is much riskier than in-vitro maturation. With maturation, the technology is used to turn stem cells into ovarian support cells. This means any mistakes won’t carry forward to the baby because the ovarian support cell is discarded after the egg has matured. All it needs to do is allow the extracted egg to mature properly. In IVG, however, the egg itself comes from stem cells. This egg will go on to provide the blueprint for all the future baby’s cells and any mistakes in copying the genetic material could cause severe consequences for the baby.
The biggest risk is epigenetic. Epigenetic marks are small chemical structures on the outside of DNA which tell cells how to ‘read’ the DNA. Marks are very sensitive to environmental stressors and so could change during the IVG process in unpredictable ways. Seemingly small changes in epigenetic marks could have dire consequences for the developing embryo.
Exposing cells in culture to cocktails of proteins to induce their development will clearly not be enough to ensure the proper deposition of these sensitive epigenetic marks. CRISPR, a well known DNA editing method, could potentially fix this. If we are ever going to consider this in humans, extensive trials on other species will have to be carried out first.
But the higher risks of IVG also come with higher rewards. If companies like Conception are successful, we will be able to completely side-step the egg collection and freezing process. This technique could open up countless new opportunities. Not only would it allow women of advanced ages to conceive, but it would also enable same-sex couples to have children that are genetically related to both partners.
Delaying aging to delay egg aging
All of the approaches discussed so far have involved manipulating the egg outside the woman’s body. Another way to expand the female reproductive window is by delaying egg aging itself. There are good reasons to favor this approach as opposed to egg freezing or in vitro gametogenesis. Firstly, compared to egg freezing, it could be far less invasive. Secondly, unlike in vitro gametogenesis, it would not risk introducing genetic and epigenetic defects through extensive cellular manipulation.
There could be other positive spillovers. Delaying egg aging might postpone the onset of menopause. As a woman’s eggs are depleted, the ovaries send out fewer chemical signals, and she goes through menopause. Menopause then brings on age-related diseases such as dementia, cardiovascular disease, and osteoporosis. Women who experience menopause earlier in life or due to surgical removal of their ovaries face even higher risks for these chronic conditions, suggesting that functioning ovaries have a health-protective effect, and later menopause correlates with increased longevity. These observations have led some in the field to contend that delaying menopause would also improve women’s health span.
Unfortunately, we are still quite far away from knowing how to achieve this. To the extent that advances have been made, they are usually merely translations of insights from the broader field of aging. An example is the recently launched VIBRANT trial, which attempts to assess the impact of rapamycin, a compound known to extend the lifespan of mice, on delaying menopause.
What accounts for our relative lack of knowledge when it comes to female reproductive aging? One reason is that it’s difficult to study the female reproductive system: as with many other elements of human health, we cannot carry out experiments ethically, so we are forced to rely on observational evidence that is often causally uncertain and deeply unreliable, or on studies done on other animals. But the female reproductive system is unusual in animals. Menstruation happens only in humans and a handful of other animals, mostly primates: most mammals have periods of being ‘in heat’ and do not bleed menstrually, with their uterine lining being reabsorbed if they do not conceive. Menopause is even more distinctly human: only a small handful of long-lived animals go through it.
Extending fertility to end the motherhood penalty
Over the past century, much of the world has made big strides against gender inequality in the labor market, through things like changes to cultural norms, laws against discrimination against women, and technology that has made jobs more flexible.
The next frontier is conquering the motherhood penalty, which has the dual effect of holding women back in their professional lives and stopping them from having the families they would like to have. Of course, part of this will involve policy and social change – women have basically the same biology in Sweden and South Korea, yet the motherhood penalty is much larger in South Korea. But we can go further. Technological advances that extend women’s fertility windows give women the option to invest in their careers in their thirties and have children later. A hundred years from now, women having children well into their forties may be as commonplace as married women and mothers in the workforce are today.