SGLT2, a protein in the kidney, takes glucose out of the urine and puts it in the blood. Blocking this reduces diabetes, heart disease, and kidney disease – but we’re not exactly sure why.
Most drugs get approved to do one thing. In rare cases, drugs get multiple indications, allowing their manufacturers to advertise them as treatments for a range of conditions. Sodium-glucose cotransporter-2 (SGLT2) inhibitors, also called flozins, began as diabetes drugs. Surprisingly, they turned out to also be very effective at improving heart health. Then they were discovered to slow the progression of chronic kidney disease, one of the leading causes of death and disability worldwide. Preliminary evidence indicates that they show promise in helping several other conditions, but no one knows exactly how they achieve this yet. Could SGLT2 inhibitors be a new medical Swiss Army knife?
The backstory of flozins
SGLT2 is a protein found in the kidneys that stops the body from wasting calories. It works like a pump that extracts glucose from urine and moves it back into the blood. The sodium in the name refers to how that pump is powered: like a water wheel using a gradient in water height to move machinery, SGLT2 uses the gradient in sodium concentration between the urine and the blood as an energy source.
Phlorizin was the first drug that blocks SGLT2 to be isolated, in 1835. This compound was extracted from the root bark of the apple tree by French chemists and studied in the hopes that it would be useful for stopping fevers. It wasn’t.
It took a long time before anyone found a use for phlorizin. About 50 years after its original discovery, German physician Josef von Mering discovered that it stimulates excess sugar excretion in the urine of animals. It likely didn’t strike many people at the time as a good treatment for diabetes – after all, excess sugar in the urine is a symptom of diabetes, as are some of the other effects caused by phlorizin, such as weight loss and excessive thirst. In fact, the effects of phlorizin administration in animals have in the past been called ‘phlorizin diabetes’.
The paradigmatic sign of type 2 diabetes is high blood sugar. In a healthy person, the pancreas releases the hormone insulin in response to increases in blood sugar. Insulin, in turn, tells various cells in the body to absorb the excess sugar. But when someone has type 2 diabetes, the cells do not listen as well: they become resistant to the effect of insulin and let sugar build up in the blood. This is a problem because very high blood sugar, known as hyperglycemia, causes damage to multiple organs.
In 1987, phlorizin was used to clarify the role of high blood sugar in type 2 diabetes. Researchers at Yale University found that phlorizin restored insulin sensitivity in a rat model of diabetes, effectively curing them of the disease, whereas stopping the phlorizin treatment made insulin resistance return. This showed that high blood sugar is not just a result of insulin resistance, but also plays a role in worsening it once it begins.
This kindled interest in using flozins – the name of the group of drugs that block SGLT2, also called SGLT2 inhibitors – as antidiabetic medications. But phlorizin has other effects as well. It doesn’t just block SGLT2 – it also blocks SGLT1, the main protein that’s responsible for glucose absorption in the small intestines. This blockage leads to substantial gastrointestinal side effects, like diarrhea (similar to antidiabetic drugs metformin and acarbose). Moreover, only small amounts of phlorizin are absorbed by the digestive system, meaning that patients would need to inject it or take large oral doses (and these large doses are associated with more severe side effects).
These issues created problems with the feasibility of using flozins medically. But in 2000, Japanese researchers solved the absorption problem by developing synthetic flozins that were easily absorbed into the blood after taking them orally. These drugs also increased the release of glucose in the urine, implying they were working as expected. But like phlorizin, they also blocked SGLT1, and caused the same side effects.
Soon this problem was solved too. More work by Japanese researchers on synthesizing flozins led to the development of canagliflozin and dapagliflozin, which are both absorbable and selective – blocking SGLT2 much more than SGLT1.
Meanwhile, evidence grew that indirectly supported the safety of flozins for long-term use. In the 2000s, researchers discovered the cause of familial renal glycosuria, a condition that runs in families where patients have abnormally and persistently high levels of glucose in their urine, but have otherwise normal kidney function. They also have normal blood glucose levels and life expectancies, and report no complaints related to the condition.
It turned out that familial renal glycosuria was caused by genetic mutations in the SGLT2 gene that reduced the effectiveness of the SGLT2 pump, creating an effect similar to that of flozins. The fact that people could live completely normal lives with an impaired SGLT2 gene (and thus sweeter urine than everyone else) provided evidence that flozins, which artificially mimicked the condition, could be safely used in the long run.
The diabetes trials
It was time for clinical trials. In the late 2000s, the two synthetic flozins developed by Japanese researchers, canagliflozin and dapagliflozin, were bought by Johnson & Johnson and AstraZeneca respectively, and both began clinical trials for the drugs.
These trials were for diabetes, following the train of research since the 1980s that had established that inhibiting SGLT2, and thus lowering blood sugar, can help control type 2 diabetes. But rather than looking at how the compounds affected survival or the symptoms or complications of diabetes, the trials were based on surrogate endpoints, meaning that they only had to show that they directly affected biomarkers of the disease, such as high blood sugar. Surrogate endpoints were introduced to speed up drug research and encourage more research into compounds that take a long time to impact the things we care about directly.
The results were conclusive, though unsurprising. By stopping SGLT2 from extracting sugar from the urine into the blood, both flozins directly reduced rates of hyperglycemia, which by this point was known to be a major symptom of diabetes, and also a contributory cause.
The heart trials
After flozins were approved as diabetes drugs, on the basis that they lower the markers of diabetes, they had to go through further trials to be sure that they did not increase the risk of heart attacks, strokes, or deaths due to cardiovascular disease. This requirement was imposed by the FDA in 2008, after a meta-analysis published in 2007 found that rosiglitazone, another diabetes drug approved on the basis of surrogate endpoints, increased the risk of heart attacks by 43 percent.
These trials were imposed to confirm the benefits of the drugs were not outweighed by cardiovascular side effects.
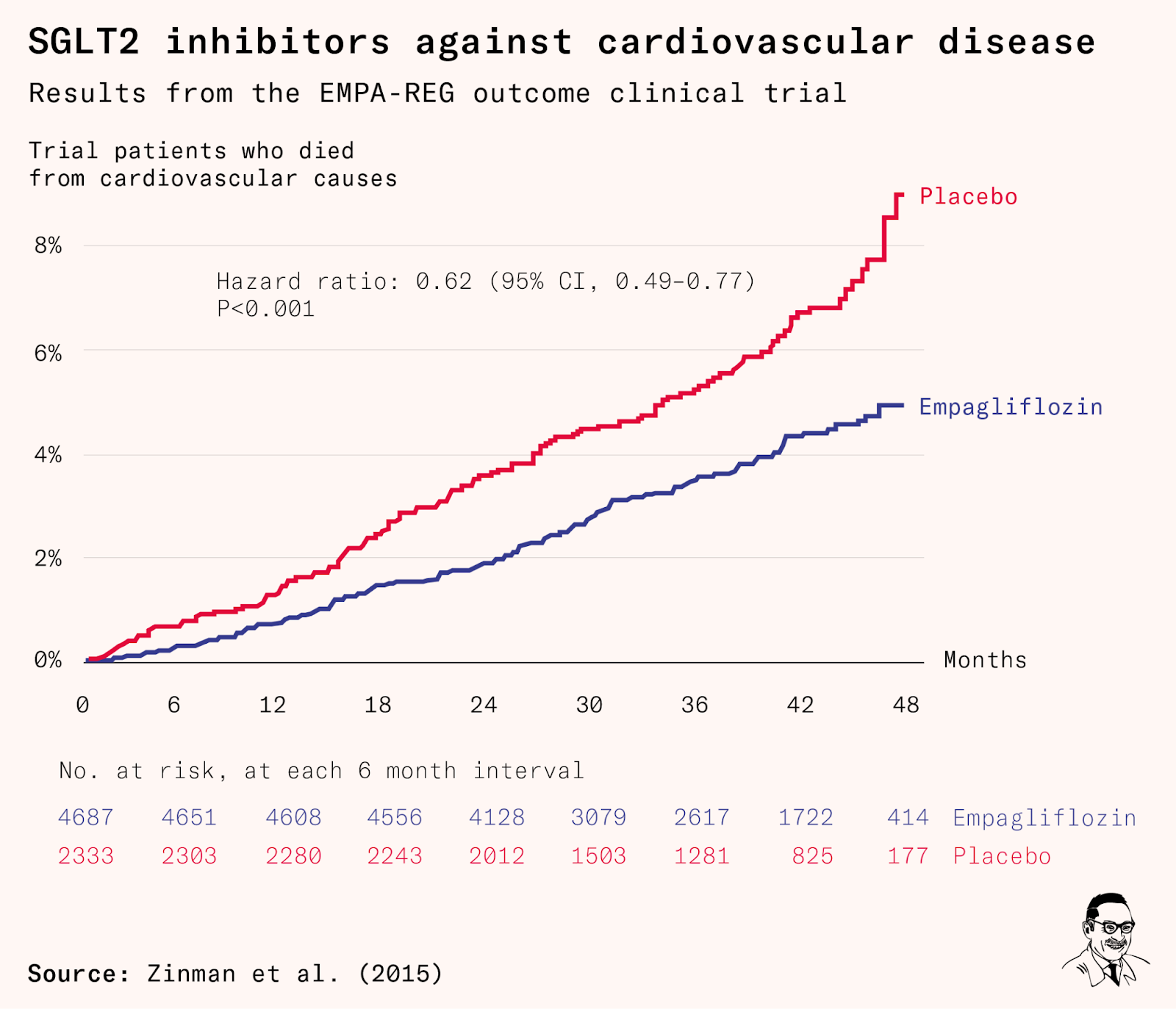
Yet something unexpected happened: the trial for empagliflozin – which, like dapagliflozin and canagliflozin, inhibits SGLT2 much more strongly than SGLT1 – showed a 14 percent reduction in major cardiovascular events, a 35 percent reduction in hospitalizations for heart failure, and a 38 percent reduction in cardiovascular deaths overall – all statistically significant.
Other flozins followed suit, backing up their diabetes trials with heart health trials. Not only did they get to stay on the market as antidiabetic drugs, but between 2020 and 2023, the FDA gave three of them indications for heart failure as well.
As discussed, SGLT2 is a protein primarily found in the kidneys which prevents sugar and sodium chloride from being passed into the urine. It is obvious how the inhibition of SGLT2 decreases blood sugar, making flozins good medications for type 2 diabetes. But we’re not sure why they’re so good for the heart.
We know that flozins reduce blood pressure, but this effect is small – nowhere near enough to account for their protection against heart diseases. Conventional blood pressure therapy reduces the risk of heart failure by 28 percent for every 10 millimeters of mercury (mm Hg) decrease in blood pressure. But in one of the large flozin trials mentioned above, patients on canagliflozin had 39 percent lower rates of heart failure despite blood pressure reductions of only 3.5 mm Hg – almost three times the ratio of heart failure reductions to blood pressure reductions. Post hoc analyses of the same trial found that the blood pressure–lowering effect of canagliflozin explained only four percent of its effect on kidney function.
It similarly has been found that the cardiovascular benefits of flozins cannot be explained by their effect on blood sugar alone.
There have been a whole range of additional proposed explanations, including the fact that the drugs increase diuresis (urination) and natriuresis (salt passing through to the urine); or that they improve cardiac energy metabolism, potentially encouraging the heart to fuel itself with lipids.
Kidney disease: one of our biggest problems
A tenth of the world’s population has chronic kidney disease. About a million people died from it last year. If it happens to you, it will begin with your kidneys removing waste from the blood less efficiently than they do in healthy people. The disease often starts silently, without noticeable symptoms. It’s often detected through routine blood tests that show higher levels of waste products in your blood. When your disease gets worse, however, you can start feeling quite ill. Your body might begin to swell up because it is holding on to more fluid than it should, which also leads to higher blood pressure and even damage to the heart. As waste products build up in your blood, you may feel tired, weak, and less sharp mentally.
At advanced stages of the disease, your bones become weaker and more prone to fracture. You might feel muscle weakness and fatigue. As the condition progresses, you might lose your appetite, leading you to lose weight without trying, and your muscles might begin to waste away. If the disease progresses to the last stage, called end-stage kidney disease, to survive you will need regular dialysis – an extremely time-intensive, costly, and painful process that ultimately only alleviates the symptoms rather than the underlying problem – or a kidney transplant.
For about two decades, there have been relatively minor changes to treatment guidelines for chronic kidney disease. The last major change was in 2002, when the National Kidney Foundation released clinical practice guidelines for chronic kidney disease that recommended two types of drugs – angiotensin-converting enzyme (ACE) inhibitors and angiotensin receptor blockers (ARBs) – as some of the main therapies to slow the progression of kidney disease in patients. This represented meaningful progress – before these drugs became widely available, clinical guidelines largely focused on the treatment of end-stage kidney disease after its onset rather than on its prevention.
But those drugs are not very effective for all patients, being more effective for a subset of chronic kidney disease patients who have excessive protein leakage than for those who don’t.
And the burden of the disease is still large and rising. Around 130,000 people in the United States develop end-stage kidney disease each year, and more than 800,000 people have the condition. Because the population has been growing older, these numbers are rising, and the demand for kidneys for transplantation far outstrips the supply. The number of patients on the waiting list continues to grow, and many patients who would likely want a transplant never get added to the waiting list in the first place.
The kidney trials
Initially, there was concern that flozins might harm regular kidney function. Diabetes patients in trials had a small increase in serum creatinine, a biomarker of the filtration rate of small blood vessels in the kidneys, which seemed to suggest the signs of a problem.
Instead, more trials found that, over longer time horizons, treatment with flozins reduced the progression of kidney disease for those with diabetes – in fact, flozin treatment was dramatically superior to placebo: patients given empagliflozin, for example, had a 39 percent lower risk of getting new or worsening kidney disease than the placebo group.
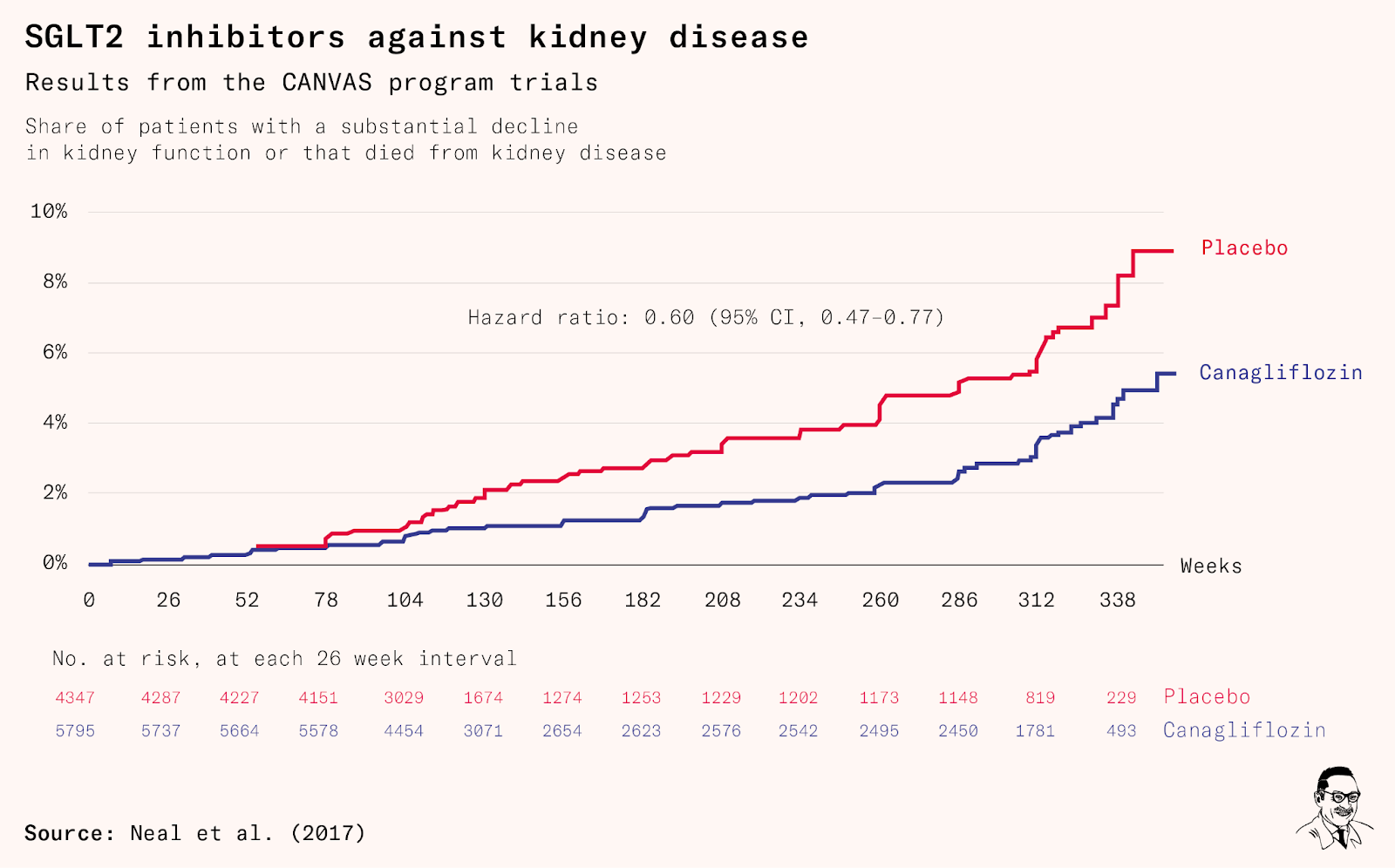
Another major trial, this time testing canagliflozin, with over 10,000 patients with type 2 diabetes, found a 40 percent risk reduction in a composite outcome measuring worsening kidney function, and a 14 percent reduction in major cardiovascular events (such as heart attacks or strokes) or death.
In the meantime, pharmaceutical companies were willing to put in yet more resources on further trials of patients with kidney disease but without diabetes, to see if they could have these drugs approved to treat a wider range of patients.
In 2020, the first major trial to test flozins on patients with or without diabetes also had dramatic results: chronic kidney disease patients who were given dapagliflozin had a 36 percent lower risk of developing end-stage kidney disease. Almost all the patients in the trial were already taking effective medications for their disease; meaning that this improvement was above and beyond the benefits of their current medication.
By the following year, the FDA approved dapagliflozin for the treatment of chronic kidney disease in both diabetic and nondiabetic patients – in addition to the approval for both heart failure and diabetes.
The mystery link between flozins and kidneys
The mechanism behind the benefits of flozins to kidney function is not fully understood.
One possible explanation for why flozins are effective at preventing kidney disease in diabetic patients is because, in their absence, some kidney cells are overburdened as they try to filter sugar out of the blood.
Chronic kidney disease typically starts when a condition – such as diabetes, hypertension, or lupus – causes damage to part of the kidneys. To compensate for this damage, other cells start working extra hard to filter blood, leading to what is called relative glomerular hyperfiltration, which describes excessive filtration in some parts of the kidneys.
Initially, this can help maintain someone’s overall kidney function despite damage from their disease. But with time, the overworked remaining kidney cells start to suffer. This can mean that chronic kidney disease continues to worsen even after the other clinical condition that initially caused kidney damage is brought under control.
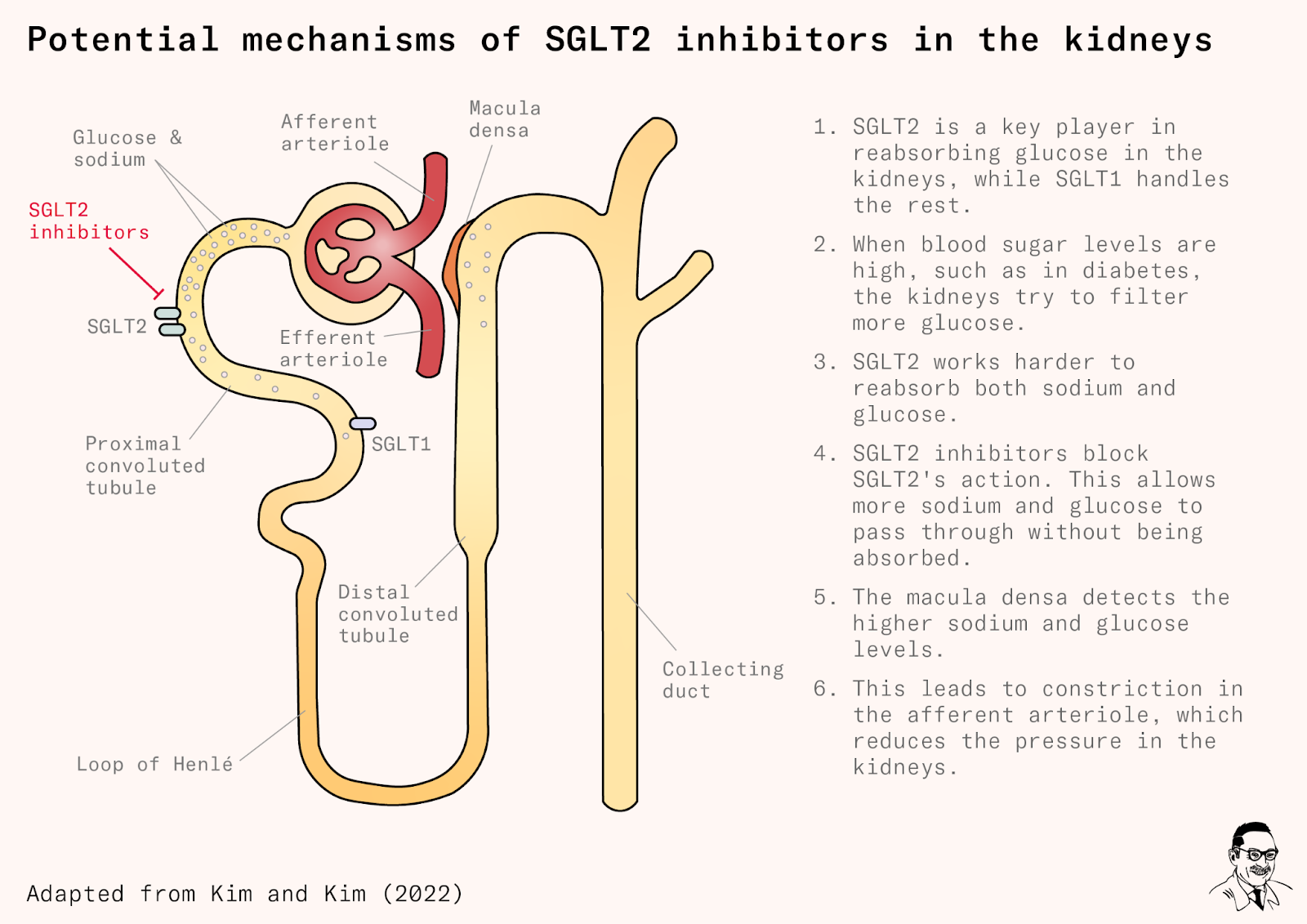
Flozins might protect the kidney by reducing this process of overwork by surviving kidney cells. When patients take these drugs, more sodium passes along those cells, instead of being filtered out along with the extra glucose. Special cells in another part of the kidneys, called the macula densa, respond to the extra sodium and constrict blood vessels that are channeling blood into the kidneys, which reduces the pressure in the kidneys, and is speculated to be protective.
This may be part of the reason these drugs also protect the heart, since poor kidney function can lead to excess blood in the heart, or volume overload, which makes it harder for the heart to function normally.
Although previous kidney disease drugs, like ACE inhibitors and ARBs, also have benefits for heart function, there is no consensus on why specifically these drugs have such large beneficial effects. But their effects have been sufficiently large that these drugs have been used to treat heart failure as well. Flozins carry on this tradition of repurposing kidney drugs to treat heart diseases.
The potential of flozins
Overall, the potential of flozins is large. Nearly a million unique patients get hospitalized for heart failure each year in the United States. If half of those at risk were to take empagliflozin, perhaps 150,000 fewer people might be hospitalized for the condition each year, assuming the results of the two biggest trials can be extrapolated to the rest of the population. Millions more are hospitalized across Europe and around the rest of the world.
In the United States, there were over 130,000 new cases of end-stage kidney disease in 2019 alone. Assuming that dapagliflozin is as effective in the wider population as it was in a clinical trial and that its effects don’t diminish over time, a broad rollout of dapagliflozin could lead to tens of thousands fewer people developing end-stage kidney disease each year in the country. In comparison, only around 25,000 kidney transplants are performed each year in the United States. But unlike most kidney transplant recipients, those patients would never have to see their health decline enough that they have to spend hours per week connected to a dialysis machine in the first place.
Broader effects
Recent exploratory research has suggested that flozins might also have benefits on a range of other diseases – liver disease, dementia, and respiratory diseases – which could each be important areas for future trials.
Post hoc analyses of human trials have suggested that they might improve liver function in patients with nonalcoholic fatty liver disease. In an analysis of national data from Taiwan, researchers found that SGLT2 inhibitor treatment was associated with a lower incidence of dementia. They may also reduce sleep apnea, asthma, chronic obstructive pulmonary disease, some infections like pneumonia, varicose veins, and even gout.
The fact that flozins have positive impacts on some of the most common age-related diseases that affect us might make you wonder if flozins can be conceptualized as slowing down aging, rather than only treating a narrow set of diseases.
The National Institute on Aging’s Interventions Testing Program (ITP) funds studies attempting to increase the life span of genetically heterogeneous mice with various compounds. It has a roundup of all these trials. Compounds like aspirin, resveratrol (in red wine), curcumin, green tea, medium-chain triglyceride oil, fish oil, metformin, and many more have no effect in these studies, despite huge amounts of media hype.
Despite that context, an ITP-funded study found that canagliflozin extended the median survival of normal male mice by 14 percent (without affecting the survival of female mice). A more recent replication saw life span increase by 4.6 percent in inbred male lab mice – smaller, but still impressive by the standards of other life span extension drugs.
This is interesting because the causes of natural death in these lab mice are very different from those in humans. Unlike humans, mice studied in the ITP almost all die from cancer; they do not develop diabetes naturally, and they very rarely die from kidney or cardiovascular disease.
This makes it one of the most promising antiaging drugs studied by the ITP – one pharmaceutical researcher ranked it as third most promising after rapamycin and acarbose, another antidiabetic drug. Acarbose works by preventing the body from producing amylase, the enzyme we use to digest most carbohydrates. Because acarbose prevents digesting them, those carbohydrates instead pass through the stomach and small intestine to the large intestine, where they effectively function as fiber, and are digested by the body’s resident bacteria. In about a third of patients, this causes such severe bloating, cramps, and diarrhea that they discontinue taking the drug. But the upside is that acarbose mechanically reduces blood sugar spikes – potentially implying a similar mechanism of life extension to flozins, if it holds up.
Maybe it will turn out that flozins do not have any special effect on slowing down aging in healthy humans. But still, it is such an intriguing prospect that is likely to see much more research.
Downsides and side effects
Even if flozins were, hypothetically, proven to be helpful in healthy people, one major reason they are unlikely to be rolled out that broadly is that, like acarbose, they have meaningful side effects.
Flozins increase the risk of genital infections, since the high concentration of sugar in patients’ urine creates a good environment for pathogens to thrive. The incidence of such infections has been found to be up to 14.5 percent in some trials, though they are mostly mild to moderate urinary tract infections, or yeast infections.
Sugary urine has another downside: it could get those providing a urine sample in trouble. Police sometimes take weeks to analyse a sample from a drunk driving case. Urine from a patient taking empagliflozin fermented into ethanol while sitting at room temperature, meaning it gave a false positive for an alcohol screening, in a recent medical case report from Philadelphia.
Occasionally, patients taking flozins face euglycemic diabetic ketoacidosis. Ketoacidosis is a condition in which blood becomes dangerously acidic due to the excessive production of ketone bodies, an alternative energy source to glucose, produced by the liver in periods of low carbohydrate intake or due to certain medical conditions. It’s unsurprising this happens: flozins essentially simulate low carbohydrate intake by decreasing the uptake of glucose by cells; this becomes a problem when it goes too far. The condition is different from most cases of diabetic ketoacidosis because blood sugar levels remain normal; this often presents a diagnostic challenge in the emergency room because doctors often expect ketoacidosis in diabetic patients to go along with high blood sugar. If doctors aren’t recognizing or noticing it, patients may be waiting longer for them to treat it.
The condition is rare, and the mortality rate of euglycemic diabetic ketoacidosis is only known roughly, but in one study of 9,940 patients with type 2 diabetes taking flozins, 25 patients developed this condition, and one of them died in the hospital (18 developed typical hyperglycemic ketoacidosis). Flozin therapy makes it 3.7 to 7 times more likely that people develop diabetic ketoacidosis, and most of those cases are euglycemic, with an absolute risk of approximately 0.1 percent each year you are on the drug. The condition is much more common among those with type 1 diabetes, for whom flozins are not approved in the United States.
An even rarer but more concerning complication, also caused by sweeter urine feeding infections in the genital area, is Fournier’s gangrene, which causes large patches of skin in the genital area to die. Around a tenth of those who get it die. This complication is too rare to have shown up in clinical trials and it is hard to get a precise estimate of its incidence. The FDA received 12 confirmed reports of the disease in patients taking flozins in the roughly five years between March 2013 and May 2018, out of a few million patients who’d received a prescription for such a drug. In comparison, they received reports of only six cases of this disease in association with other antidiabetic drug classes in the past 30 years.
But most of these issues are rare, and most patients seem to tolerate these drugs well. The discontinuation rates in human clinical trials are similar between patients on those drugs and those on placebo.
Conclusion
Whatever we discover on greater use of those drugs, flozins are extremely promising in treating diseases that affect hundreds of millions of people. Overall, these drugs change the outlook of patients with some of the most common chronic diseases, saving many from early death or disability, and show promising signs that they might do even more.

Subscribe for $100 to receive six beautiful issues per year.